By Sustainable Development for Environment Initiative (SEDI), Nigeria
 International Pollutants Elimination Network (IPEN) What is a pesticide?
International Pollutants Elimination Network (IPEN) What is a pesticide?
A pesticide is any substance, or mixture of substances of chemical or biological ingredients intended for repelling, destroying or controlling any pest, or regulating plant growth. [1]. Pesticides can also be used as vector control and agriculture control agent in public health programmes [2]. The group includes herbicides, insecticides, and fungicide so. Pesticides may be used for crops on the field, harvested produce, agricultural commodities or animal feeds and fish, 2.1% of pesticides used in the world come to Africa [3]. The cost of labor, choice of pesticide application, and the promise of swift pest control have made the use of pesticides judicial or rampant all over the world [4]. A survey on pesticides usage in Nigeria indicated that annually about 15,000 metric tons of pesticides comprising about 135 pesticide chemicals marketed locally under 200 different produce brands and formulation were imported during 1983-1990 thus making Nigeria one of the largest pesticides users in sub-Sahara Africa [5].
More than 95% of the applied herbicides and 98% of insecticides reach non-target soil micro-organisms than their target pest, as they are sprayed proportionately across the entire field, irrespective of the affected areas [6]. Hence, of the total quantity of applied pesticides, about 0.1% reaches the target organisms while the remaining quantity pollutes the soil and environment. There are 25 million occupational pesticide poisonings each year among agricultural workers in developing countries alone [7].
What are highly hazardous pesticides (HHPs)?
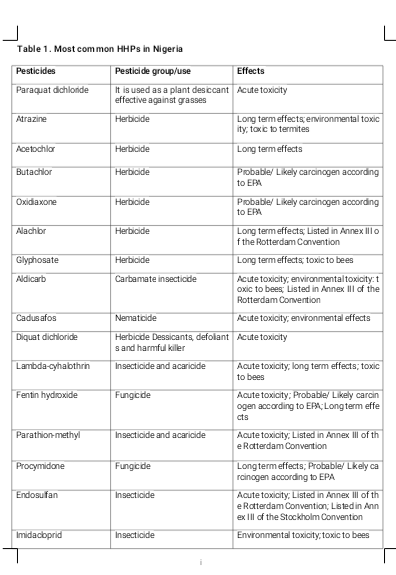
Pesticides are inherently hazardous, and among them, a relatively small number of Highly Hazardous Pesticides (HHPs) cause disproportionate harm to environment and human health including: severe environmental hazards, high acute and chronic toxicity [8]. Pesticides that appear to cause severe or irreversible harm to health or the environment under conditions of use in a country may also be considered to be and treated as highly hazardous”.
Stakeholder reflection on the failure of existing pesticide controls to reduce the incidence of damage to yhuman health and environment led FAO and WHO to launch a new initiative for a progressive ban on Highly Hazardous Pesticides (HHPs) in 2006. The HHP initiative recognizes that WHO Class II pesticide active ingredients (‘moderately hazardous’ in terms of acute mammalian toxicity as determined in laboratory testing), such as endosulfan, paraquat and chlorpyrifos, can be as problematic in reality as the ‘extremely’ and ‘highly’ hazardous pesticides which make up WHO Class I. This conclusion is also drawn from PAN’s poisoning cases data in West Africa [9] and locust cost externality assessment in Senegal [10]. In 2009 PAN International published its ‘List of Highly Hazardous Pesticides’ as a contribution to UN discussions [11]. It provides a catalogue of the most harmful pesticides that is more comprehensive, and takes into account more potential pesticide hazards, than current listings by official bodies.
HHPs are considered to represent a fraction of all registered pesticides worldwide; in some cases as small as 6 percent (Southern African countries) while in other cases as high as 30 percent of the registered products [8]. They are still in use in many low and middle income countries because of inadequate regulation and monitoring and are primarily used in agriculture and in public health (DDT and Clothianidin) for malaria vector control, but also used in domestic gardens. They have been detected in air, water, soil, animals and humans and have been found in local food systems and global food commodities such as bananas, coffee and rice, but the most contaminated crops are fruits and vegetables. They can also cause loss of biodiversity, kill fish and birds and poison wildlife. Therefore, HHPs should be progressively phased out by more sustainable alternatives.
Impacts of HHPs
The impacts of the highly hazardous are divided into human health and environmental impacts.
(A) Human health impacts
Human health effects can be acute or chronic poisoning, linked to a range of serious illnesses and diseases from respiratory problems to cancer. Exposure can occur in many ways. Farmers and farm workers can be exposed through the treatment of crops, plants and grain stores. Rural residents living next door to farms can be exposed to pesticide drift or from contaminated air and ground or surface water. Consumers of food crops sprayed with pesticides can be exposed through pesticide residues. Consumption of crops and plants grown under chemical pest control like fruits and vegetables without proper washing for example, [13] reported the presence of paraquat residues in some commonly consumed vegetables in Abeokuta, Nigeria. However, no direct health impact was reported in the study.
Acute poisoning
Acute poisoning means that they can cause harmful or lethal effects after a single episode of ingestion, inhalation or skin contact. The symptoms are evident shortly after exposure or can arise within 48 hours. This can include:
- respiratory tract irritation, sore throat and/or cough
- allergic sensitisation
eye and skin irritation
- nausea, vomiting, diarrhoea
- headache, loss of consciousness
- extreme weakness and or ultimate death.
- Chronic or long-term poisoning
These are harmful effects over an extended period, usually following repeated or continuous exposure at low levels, can be very serious illnesses. They are linked to the development of Parkinson’s disease; asthma; depression and anxiety; attention deficit and hyperactivity disorder; and cancer, including leukaemia and non-Hodgkin’s lymphoma.
Environmental impacts
1. Impact on aquatic organisms: Pesticide drifts or residues lead to deterioration of water quality, hence reducing the number of aquatic organisms.
2. Water pollution and contamination: Spraying or use of hazardous pesticides and incorrect pesticides application approach adjacent to drinking water resources may lead to their contamination, and could result to pollution of surface and underground water.
3. Soil degradation / contamination: Long-term excessive use of pesticides will cause higher pesticide resistance and pesticide residues in the soil which will cause soil contamination.
4. Extinction of non-target species: impact on the non-target species (bees, natural enemies, etc.).
5. Air pollution: Poor handling, application and disposal of pesticides products such as empty containers and obsolete products will cause air pollution.
6. Soil fertility imbalance: Pesticides cause imbalance of soil fertility which directly affects crop yield.
 Pesticide going to the soil during application (Photo credit to SEDI. Location –Edo State, Nigeria)
Pesticide going to the soil during application (Photo credit to SEDI. Location –Edo State, Nigeria) Effects of using specific HHPs
There is certainty that the application of Endosulfan pesticide is moderately persistent in Ibadan soil and hinders availability of some soil nutrients [14]. There was 85% population reduction of nematode as a result of Endosulfan application. Total DDT and heptachlor found in Ibadan ground water exceeded the WHO limits for these chemicals in drinking water [15].
Unintended costs incurred in using HHPs
The UN Food & Agriculture Organization (FAO) analyzed externalities caused by spraying high concentrations of organophosphate insecticides (mainly malathion and fenitrothion) for locust control operations in Senegal during the last outbreak in 2003 - 2005 [8]. It estimated external costs of over 8 million Euros including: 2.75 million for environmental costs; 2.5 million on human health; 2.1 million in agricultural production losses; and 0.7 million in damage prevention costs.
Unintended costs of using HHPs include:
1. Increased cost of production: The use of HHPs in agricultural farming systems leads to an increase in cost of production due to the fact that these pesticides are expensive.
2. Maintenance cost: maintenance of sprayers such as power driven models with motor and hand operated sprayers. Hand operated sprayers such as Lancet, Falcon, Knapsack, Motorized mist blower, Ultra Low Volume (ULV), and Electrodyne sprayers need to be maintained regularly through procedures like washing and oiling with light oil to prevent corrosion [16].
3. Cost of pesticide poisoning treatment: First aid for pesticide poisoning victims and hospital bills.
4. Cost of pesticide poisoning prevention: During spraying personal protective equipment (PPE) are worn to reduce contact with the pesticide. These include coveralls, long rubber gloves, goggles, respirators, rubber boots and waterproof hat. These PPE are usually expensive and increase the cost (unavailable in some cases or places when needed).
5. Environmentally pollution: The use of HHPs causes environmental degradation and pollution [16].
Applying pesticides without wearing PPE. (Photo credit to SEDI. Location –Edo State, Nigeria)
References:
[1] FAO/WHO, 2016. The International Code of Conduct on Pesticide Management - Guidelines on Highly Hazardous Pesticides. ISBN 978-92-5-109187-6.
[2] WHO, 1990. The public health impact of pesticides use in agriculture. World Health
Organization, Geneva.
[3] Food and Agriculture Organization of the United Nations. 2019. FAOSTAT Statistical
Database; FAO: Rome, Italy.
[4] Bahadur, S., Verma, S.K., Prasad, S.K., Madane, A.J., Maurya, S.P., Gaurav Verma, V.K.,
Sihag, S.K. 2015. Eco-friendly weed management for sustainable crop production-A review.
Journal of Crop and Weed 11: 181–189.
[5] Osibanjo, O.; Ikem A.; Sridhar, M.K.C. and Sobande A. 2002. Evaluation of groundwater quality characteristics near two waste sites in Ibadan and Lagos, Nigeria. Water, Air and Soil Pollution 140 (1-4): 307-333.
[6] Miller, G.T. 2004. Sustaining the Earth; Brooks/Cole: Monterey County, CA, USA; ISBN
9780534400880.
[7] Jeyaratnam, J. 1990. Acute pesticide poisoning: a major global health problem. World Health
Statistics Quarterly 43: 139-144.
[8] FAO and WHO. 2019. Detoxifying agriculture and health from highly hazardous pesticides
– A call for action. Rome.
[9] PAN UK, 2008. Hazardous pesticides and health impacts in Africa. Food & Fairness briefing
no. 6, London. Via http://www.pan-uk.org/Publications/
[10] Leach, A., Mullié, WC, Mumford, JD and Waibel, H. (2008). Spatial and historical analysis
of pesticide externalities in locust control in Senegal- first steps. Imperial College London,
University of Hanover and FAO.
[11] PAN Germany, 2009. PAN International List of Highly Hazardous Pesticides Via
http://www.pan-germany.org/
[12] Pesticide Action Network International, 2016. PAN International List of Highly Hazardous
Pesticides - 12/2016.
[13] Akinloye O. A.; Adamson I.; Ademuyiwa O. and Arowolo T. A. 2011. Paraquat toxicity and its mode of action in some commonly consumed vegetables in Abeokuta, Nigeria. International Journal of Plant Physiology and Biochemistry 3(4): 75-82.
[14] Aikpokpodion, P.E., Lajide, L., Ogunlade, M.O., Ipinmoroti, R., Orisajo, S., Iloyanomon, C.I. and Fademi, O. 2010. Effect of Endosulfan on soil and root-knot nematodes in cocoa. Journal of Applied Biosciences 26: 1640-1646.
[15] Osibanjo, O. and Aiyejuyo, A. 1994. Organochlorine pesticide residue in foodstuff of animal origin in Nigeria. Bull Environ Toxicol 54:460-464.
[16] Ekeleme, I.Y. Dugje, F. Ekeleme, A.Y. Kamara, L.O. Omoigui, A.Tegbaru, I.A. Teli,
And J.E. Onyibe. 2008. Guide to safe and effective use of pesticides for crop production in Borno State, Nigeria. 23 pp.
(Photo credit to SEDI. Location –Edo State, Nigeria)